

















Introduction
Ureteroceles associated with a duplex collecting system may lead to obstructive uropathy, the most common genitourinary anomaly of the fetus. Although most frequently presenting as hydronephrosis, damage from obstruction is a progressive process which may even develop into bilateral renal dysfunction. Antenatal intervention for preservation of fetal renal function may be considered, but must be balanced against procedural risks. Therefore, accurate documentation of the progression may be necessary. Postnatal evaluation of the infants confirmed the antenatal findings. The importance of serial evaluation of fetal obstructive uropathies is dramatically illustrated
Case Prepared by Dr. Tulika Tayal – Clinical Research Sellow
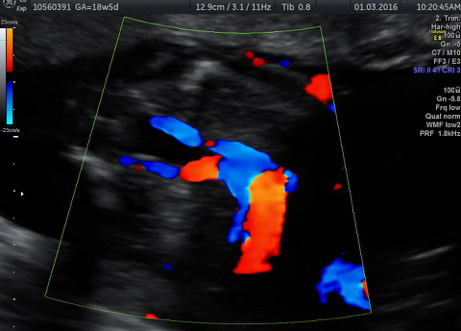
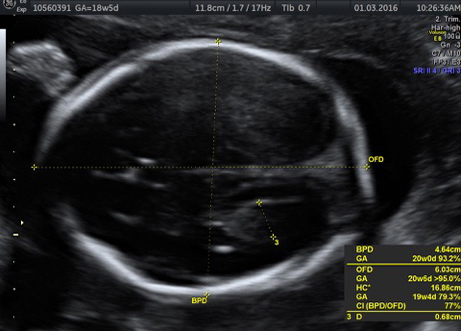
A 21 years old primigravida was refered at 20 weeks and 4 days with fetal renal abnormality for further evaluation and management . A detailed scan showed moderate left renal hydronephrosis ( Fig 1) and mild right renal hydronephrosis (Fig 1). Uretrocele was clearly noted in the bladder (Fig 2 ) .The bladder ,ureters and renal cortex , appeared normal .Amniotic fluid and fetal growth were in the normal range. There was no evidence of a double collecting system on either side or any other associated abnormalities.
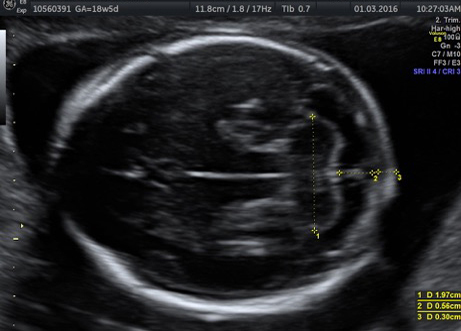
The parents were counselled that we expected a good long term outcome in this pregnancy and at present there was no need for antenatal intervention .She was advised to come for serial scans in the Renal Clinic where joint consultation with the paediatric urologist was possible. On follow up scans at 28 weeks (fig 3) , 32 weeks (fig 6) ,34 weeks(fig 7 ) scans there was progressive increase in the left hydronephrosis with no deterioration in the right kidney appearances and good amniotic fluid (fig 5). The 37 weeks scan suggested a further increase in the left hydronephrosis (fig 8.) with the right sided renal pelvis starting to show signs of obstruction(fig 9).
As the fetus was of a good weight with a good chance that neonatal cystoscopy and deroofing of the ureterocele would be possible at this stage and to prevent further renal functional damage in the left kidney ,a decision to deliver was taken. The fetal growth and amniotic fluid continued to remain in the normal range.
A male baby of 3 kg with Apgar scoring of 9/10,9/10 was delivered.
Post natal Day 1 USG,KUB ,MCU showed a very large ureterocele with bilateral hydronephrosis Day 2 DMSA scan done as a baseline for future prognosis and it revealed a normal functioning right kidney and slight impaired cortical uptake in left kidney (fig 10). Cystoscopy was done on Day 3 and large ureterocele noted extending right into the bladder neck which precluded further cystoscopic intervention.Open deroofing of ureterocele with DJ stenting was done. The stent was removed at 4 weeks when a check cystoscopy showed normal ureteral openings .The baby is well and passes urine normaly
Discussion The ureterocele results from submocosal cystic dilation of the distal ureter (ureterocele)

and is four times more common among females . This may present as intravesical or extravesical dilation with or with out hydroureter or hydronephrosis. Often associated with duplex kidneys (ectopic ureterocele), the upper moiety of the involved kidney may show associated stasis along with hydroureter. This case was showing no definite evidence of duplex kidneys. .The antenatal diagnosis of ureterocele by ultrasonography is more specific, if the classical sign of ‘a cyst with in a cyst’ is defined . If the fetal bladder is empty, the diagnosis is likely to be missed Ureterocele shows a predilection for the left side with bilateral involvement in 10 – 15 % . The differential diagnoses may include ectopic ureter, prolapsed ureter, bladder diverticulum, mesonephric duct cyst and urethral polyp. A detailed postnatal work up including scintigraphy is necessary for proper evaluation to avoid future renal complications and necessary intervention at an appropriate time.
 Fig-I showing left hydronephrosis at 20+4 weeks  Fig-II showing ureterocele at 20+4 weeks.  Fig-III showing progressive hydronephrosis of both kidneys at 28 weeks 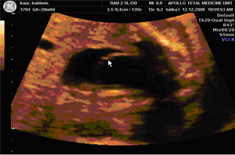 Fig-IV showing increased ureterocele at 28 weeks |


