

















Cleft lip is a condition in which the fetus’s upper lip does not join completely, causing an opening on one or both sides of the lip. The size may vary from a tiny slit to a much larger defect that goes into the nose. Rarely, the opening is in the middle of the lip.
Cleft lip and cleft palate are called orofacial clefts, which is one of the most common groups of birth defects. Cleft lip may occur alone or with cleft palate. The cause is generally not known, but heredity and exposure to certain substances, including alcohol or tobacco, may increase the risk.
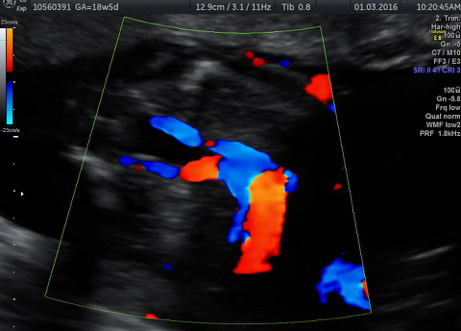
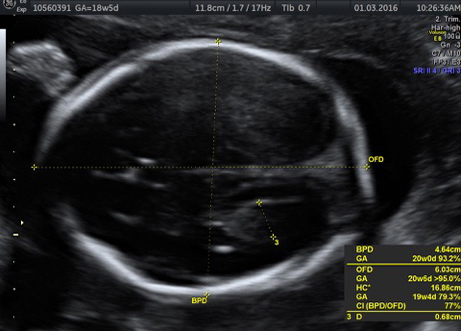
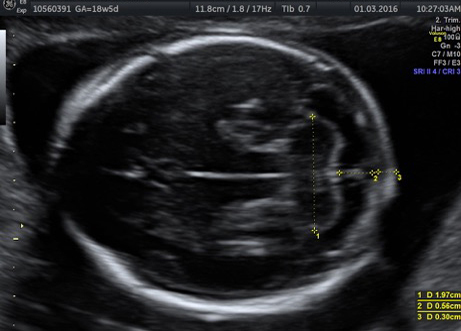
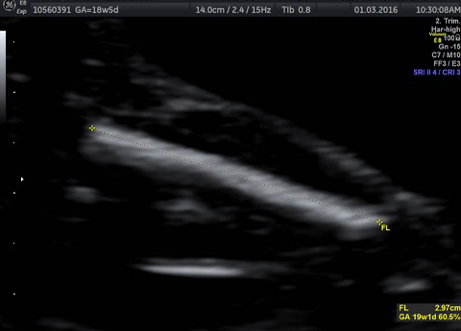
While cleft lip may be found prenatally by routine ultrasound, it usually is diagnosed at birth.
Treatment for cleft lip depends on several factors. Usually surgery to repair the defect is performed before the baby is 4 months old. Additional surgeries, as well as treatment for hearing or speech problems, may be needed.


