

















Intra fetal Laser ablation of blood supply to acardiac twin
26 year old primigravida was referred at 18 weeks and 6 days gestation with monochorionic, diamniotic twin gestation complicated by TRAP sequence 0n 17 April 2008.
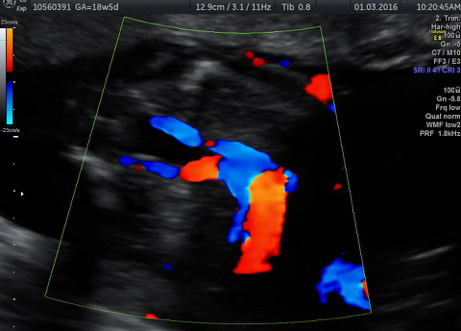
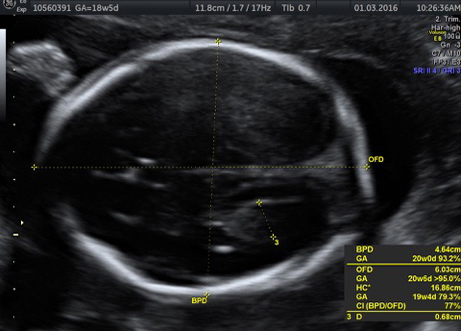
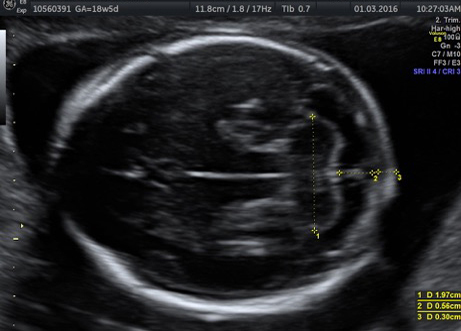
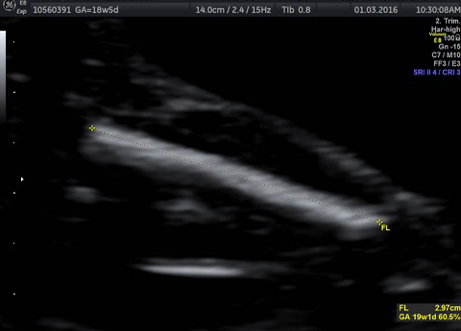
Twin A, pump twin was structurally normal but had significantly increased amniotic fluid volume (polyhydramnios), Twin B was acardiac with blood flows seen in the paravesical arteries. This twin had lower limbs which were moving.
 Twin A  Twin B  Twin C |
Pregnancy management options were discussed. These included termination of the pregnancy as there was a high probability of cardiac failure in the pump twin, as the pregnancy continued, expectant management without intervention allowing nature to follow its course with expectations of early delivery and possible cardiac complications in the pump twin, or interruption of the blood supply to the acardiac using intrafetal laser treatment to ablate the blood flow within acardiac twin.
The parents opted for laser ablation once early changes of cardiac failure were documented. The parents were aware that there is a 20 % risk of death of the co twin at the time of procedure and also of miscarriage
.
Follow up scans were done weekly to detect tricuspid regurgitation or early sign of cardiac failure in pump twin. There was progressive increase in amniotic fluid with shortening of cervix for which amniodrainage was performed at 23 wks on 6 may 2008.
At 26 wks there was signs of tricuspid regurgitation and mother was explained about the risk of cardiac failure and subsequent death
On 6 June 2008, under local anaesthesia and iv sedation and with continuous ultrasound guidance, the laser ablation device was carefully directed to where the blood supply entered the perivesical vessels of acardiac twin. Intra fetal laser using Nd: yag 400 microns/18G ablation of the tissues and blood supply in perivesical vessels was performed without complication. Color and power Doppler flow studies confirmed interruption of the blood supply to the abnormal fetus. The excess amniotic fluid volume was then removed (amnioreduction) from around the normal pump twin.
On follow up scans i.e. 23 July 2008 fetal growth was maintained but amniotic fluid appears to be reducing and is at 5th centile at 33 wks gestation and second twin appeared to be getting smaller.
At 35 wks and 5 days an emergency LSCS was done for reduced fetal movements.
She delivered live female baby with birth wt 2300 gms 0n 13 august 2008 and acardiac twin.

What is and acardiac twin or the TRAP sequence?
This is a very rare problem, happening on average once in every 35,000 pregnancies. One twin is usually completely normal. The other is body-like tissue, often with legs and a lower body, but no upper body or heart. Abnormal blood vessels on the placental surface allow the normal twin to pump blood though the tissue of the abnormal one. Because the pump twin heart has to pump for two, there is a high risk of going into heart failure. This would then lead to death of the normal twin, unless it is delivered if it is far enough along in pregnancy.
The risk of the normal or pump twin going into heart failure and dying seems to depend on the size of the acardiac. The larger the acardiac compared to the pump twin the greater the risk. The amount of blood flow into the acardiac also seems to play a role. The more blood flow the higher the risk. The harder the pump twin’s heart is working, the greater the risk of heart failure also. All of these things can be looked for with ultrasound tests.
Management Options
One option in this case is simply watching for the earliest signs of heart failure in the pump twin, with frequent ultrasounds. If heart failure is identified, and the pregnancy is far enough along then the pump twin would simply be delivered.
The other option, if the acardiac twin is large enough and we are worried about the amount of blood flow to it causing heart failure in the healthy twin is to stop the blood flow with Fetal Image-Guided Surgery (FIGS-IT). We currently do this using a thin needle, which we guide into the place where the blood vessels feed into the acardiac twin, using ultrasound. Once in place this instrument called an laser ablation device using NdYAG: 400 produces a very high local heat, to burn the tissue and destroy the blood vessels to stop the blood flow. The needle is so thin that no incision is necessary and the pain and recovery are similar to an amniocentesis


